É uma síndrome dolorosa na rótula, cada vez mais frequente nos jovens a ponto de estatisticamente serem tão numerosas nos jovens quanto as lesões mais simples nos meniscos. Ela é uma espécie de amolecimento da cartilagem da rótula pelo atrito incorreto contra os côndilos do fêmur. O desalinhamento da rótula e a sua posição mais alta que o normal são fatores predisponentes. O exame ortopédico aliado a exames radiológicos não tem dificuldade para se firmar um diagnóstico. Como sinal básico, estando o joelho levemente fletido e a coxa relaxada, quando se empurra a rótula lateralmente, aparece uma dor aguda (Teste de compressão da Patela). Quando está em seu início, o uso de antiinflamatórios, fisioterapia e repouso, costuma reverter o quadro. Em seguida iniciam-se exercícios de hipertrofia do quadríceps através de exercícios isotônicos assistidos. Outra técnica com excelentes resultados é a RPG (Reeducação Postural Global). Na técnica o paciente é mantido em posturas corretoras que se relacionam com a articulação e as estruturas músculo-esqueléticas envolvidas direta e indiretamente. A persistência da dor ou sua reagudização pode requerer a necessidade de uma cirurgia para realinhamento da rótula.
O que está acontecendo no corpo?
Quando o joelho é dobrado, a rótula desliza de cima para baixo sobre a extremidade superior do fêmur (osso da coxa). O lado interno da rótula está em contato com o fêmur. Como o resto da articulação de joelho, esta superfície é coberta por cartilagem. Cartilagem é a substância branca brilhante e lisa que também é encontrada em articulações animais. Muita tensão entre a rótula e o fêmur pode danificar a cartilagem, e a superfície em comum é amolecida e lesada. Esta condição causa irritação articular e dor.
Às vezes ocorre inchaço articular porque é produzido fluido (líquido sinovial) extra para melhorar a lubrificação. A pressão de contato entre a rótula e fêmur varia de acordo com atividade. Flexões intensas do joelho exercem uma força equivalente a cinco vezes o peso do corpo. Subir degraus equivale a três vezes o peso de corpo. Algumas pessoas têm os sintomas e achados físicos do joelho de corredor sem a patologia subjacente na cartilagem.
Quais são os sinais e sintomas da condição?
A dor acontece na porção da frente do joelho, ao redor da rótula. A dor pode acontecer com atividade, ou até mesmo depois de se sentar com os joelhos dobrados por tempo prolongado. Às vezes o joelho parecerá frouxo, embora este não é a verdadeira instabilidade de uma lesão de ligamento. O joelho pode parecer travar quando as superfícies ásperas da rótula e de fêmur prendem-se uma a outra. Isto é chamado pseudo-travamento que contrasta com o verdadeiro travamento visto numa lesão de menisco ou com um corpo estranho solto na cavidade articular do joelho.
Se a articulação está bastante irritada, o forro da cavidade articular, chamado sinóvia, pode produzir fluido extra (líquido sinovial). Fluido sinovial, em quantias pequenas, atua como óleo para lubrificar a articulação e ajudar a rótula a deslizar suavemente.
Às vezes uma roçar ou estalido da rótula contra o fêmur pode ser ouvido quando o joelho está curvando-se. A extremidade da rótula pode ser dolorosa. O joelho pode conter fluido extra (efusão ou água no joelho). Em alguns casos, a rótula tende a deslizar para o fora do joelho. Quando a dor dura muito tempo, o quadrícepis, o músculo de coxa que desdobra (estende) o joelho, pode se atrofiar (fica menor).
Quais são as causas e riscos da doença?
O problema normalmente é devido ao uso excessivo da articulação (correr muito, muito rápido, ou para cima). Condições que fazem com que o joelho fique pouco alinhado podem contribuir para a tensão extra sobre a patela: bater com o joelho ou realizar rotação interna (para dentro) do fêmur. Uma baixa posição da rótula, chamado patela baixa, ou pronação excessiva. Músculos do quadrícepis tensos podem aumentar a pressão na rótula.
O que pode ser feito para prevenir a
condição?
Exercícios de alongamento são bons para prevenção do joelho de corredor, particularmente aqueles projetados para os músculos do quadrícepis. Um programa de treinamento moderado deve evitar tensão no joelho. Devem ser evitadas distâncias excessivas, acelerações e subidas.
Como a condição é diagnosticada?
O diagnóstico é baseado nos sintomas e no exame do joelho. Radiografias são normalmente normais, embora as radiografias possam mostrar um pequeno desgaste no lado interno da rótula. Artroscopia, uma técnica que inspeciona o joelho por um instrumento tubular inseriu na articulação, pode ser diagnóstica.
Exercícios de alongamento são bons para prevenção do joelho de corredor, particularmente aqueles projetados para os músculos do quadrícepis. Um programa de treinamento moderado deve evitar tensão no joelho. Devem ser evitadas distâncias excessivas, acelerações e subidas.
Como a condição é diagnosticada?
O diagnóstico é baseado nos sintomas e no exame do joelho. Radiografias são normalmente normais, embora as radiografias possam mostrar um pequeno desgaste no lado interno da rótula. Artroscopia, uma técnica que inspeciona o joelho por um instrumento tubular inseriu na articulação, pode ser diagnóstica.
É preciso avaliar o membro como um todo, inclusive posturas e marcha; existem examaes como a baropodometria que nos ajudam muito.
Quais são os efeitos a longo prazo?
Efeitos a longo prazo são raros. Se o uso excessivo continua e são ignorados os sintomas, a artrite é uma possibilidade.
Quais são os tratamentos?
Drogas antiinflamatórias não hormonais (AINH), como naproxeno, ibuprofeno, e aspirina, podem ser usadas.
Quais são os efeitos colaterais dos tratamentos?
AINH pode ter efeitos adversos no estômago, rins, sangue ou fígado.
O que acontece depois do tratamento?
Treinamento adequado, alongamento preparatório, e possivelmente o uso de aparelhos especiais deve ser continuado.
Quais são os efeitos a longo prazo?
Efeitos a longo prazo são raros. Se o uso excessivo continua e são ignorados os sintomas, a artrite é uma possibilidade.
Quais são os tratamentos?
Drogas antiinflamatórias não hormonais (AINH), como naproxeno, ibuprofeno, e aspirina, podem ser usadas.
Quais são os efeitos colaterais dos tratamentos?
AINH pode ter efeitos adversos no estômago, rins, sangue ou fígado.
O que acontece depois do tratamento?
Treinamento adequado, alongamento preparatório, e possivelmente o uso de aparelhos especiais deve ser continuado.
Tratamento com Fisioterapia
A Fisioterapia pode auxiliar, especialmente, no fortalecimento de alguns músculos e de exercícios que enfatizam o alongamento. Músculos fortes permitem que o joelho tenha boa estabilidade, além de tornar atividades muito exigentes para o joelho, relativamente, mais leves. O treinamento de força também fortalece a cartilagem, deixando-a mais resistente aos possíveis desgastes. Mas esse tratamento fisioterapêutico deve ser sempre baseado numa avaliação detalhada de todos os fatores que podem estar relacionados ao desenvolvimento da condromalácia. O trabalho da Fisioterapia pode envolver ainda:– Programa de reeducação de movimentos, corridas e outros gestos esportivos;
– Técnicas de liberação manual do tecido;
– Técnicas articulares manuais;
– Orientações acerca das atividades e sobrecargas na patela.
A conduta fisioterapêutica deve ser, sobretudo, individualizada.
devemos evitar o avanço da lesão o quanto for possível, reestruturando e reequilibrando
a função muscular, além de adequando a série à realidade do aluno:
- Alongamento dos músculos posteriores dos membros inferiores.
- Fortalecimento do músculo vasto medial oblíquo
- Propriocepção
- Uso de bandagens e joelheiras temporariamente deve ser estudado, assim como palmilhas corretivas após baropodometria, com avaliação constantes destas palmilhas, pois as mesmas irão ceder com algum tempo.
Recomendações
– Durante o tratamento é muito importante não sobrecarregar o joelho, fazendo-o descansar para evitar os inchaços e prevenir o retorno do problema;– Para quem se exercita fisicamente, é indispensável o investimento anterior em exercícios de alongamento e o investimento posterior em exercícios de descompressão;
– Para corridas, usar tênis com um bom amortecimento;
– Evitar saltos. Seu uso poderá agravar uma condromalácia;
– Com relação ao retorno aos esportes, são recomendados treinos iniciais com intensidade leve.
Mas a correta movimentação não é referente, apenas, ao joelho. Seja em atividades domésticas do dia-a-dia, no trabalho, no lazer ou no esporte, o corpo todo deve se movimentar de forma coesa.
Garantir lugar suficiente para a perna no carro ou no seu lugar de trabalho, evitando manter o joelho flexionado mais de 90 graus por muito tempo.
- Manter boa postura e evitar cruzar as pernas por longos períodos.
- Quando estiver deitado, não deixar o peso do corpo pressionar ou mover a patela, usando um travesseiro para manter os joelhos levemente separados e as patelas no lugar.
- Usar sapatos confortáveis, principalmente durante os exercícios, o ideal é usar o tênis.
- Perder o sobrepeso ajuda muito no tratamento.
A condropatia patelar apresenta diferentes estágios, conforme o grau de degeneração da cartilagem: amolecimento, fragmentação ou fissuras, até a erosão ou perda total. Por isso há necessidade de consulta clínica imediata, ainda no início das dores. Se ocorrer insistência na atividade física, as fissuras na cartilagem podem expor os ossos à fricção, aumentar consideravelmente as dores e causar inchaço no joelho afetado. O tratamento cirúrgico é o último recurso, pois causará limitação da atividade esportiva. Outebridge (1961):
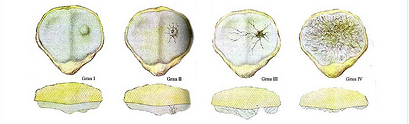
- Grau I: amolecimento da cartilagem e edemas.
- Grau II: fragmentação da cartilagem ou rachaduras com diâmetro inferior a 1,3 cm de diâmetro.
- Grau III: fragmentação ou rachaduras com diâmetro superior a 1,3 cm de diâmetro.
- Grau IIII: erosão ou perda total da cartilagem da articulação em questão, com exposição do osso subcondral.
- EXERCÍCIOS REALIZADOS 3 SERIES DE 15 E ALONGAMENTOS DE 1 MINUTO

