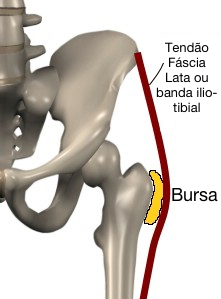
A bursite trocantérica é um processo inflamatório que afeta o líquido sinovial do grande trocânter do fêmur.
O grande trocânter do fêmur é fundamental na dinâmica dos membros inferiores
porque constitui a inserção dos músculos extensores (como por exemplo o grande
e o pequeno glúteo) e rotadores externos do quadril (por exemplo o piriforme).
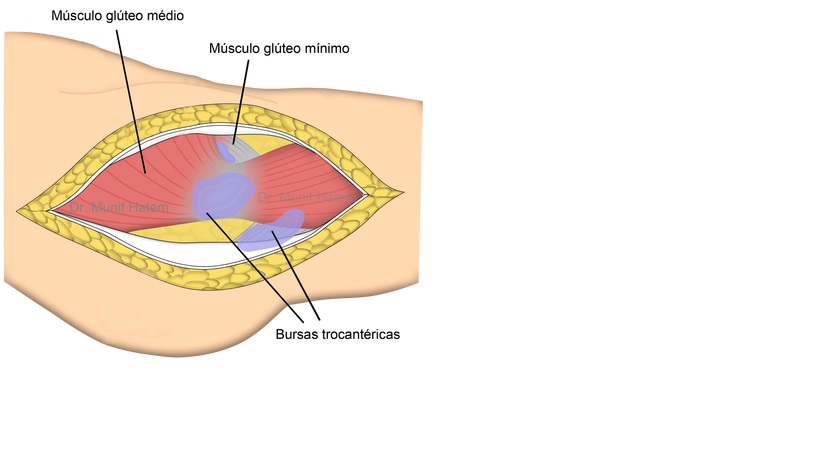
Existem três bursas sinoviais no trocânter do
fêmur, que estão:Estas bursas funcionam como se fossem um “saco vazio” sobre as proeminências ósseas, facilitando o deslizamento de tendões e fáscias sobre o osso. Bursite trocantérica é uma causa comum de dor no quadril e os pacientes frequentemente sofrem limitação nas suas atividades físicas e dormem com dificuldade.
- Entre o grande trocânter do fêmur e a fáscia lata (as mais atingida)
- Entre o tendão do grande glúteo e o osso
- Dentro do tendão do pequeno glúteo.
A bursite trocantérica afeta pessoas de meia-idade e idosos, afeta mais freqüentemente mulheres e indivíduos com desequilíbrios no corpo, por exemplo, aqueles com um membro mais curto do outro (eterometria).
Existem as mesmas chances que a bursite ocorra a direita ou esquerda, geralmente é bilateral.
A trocanterite inclui a bursite trocantérica e a entesite ou tendinite insercional dos músculos que se inserem sobre o grande trocânter, por exemplo os rotadores externos do quadril.
Esta doença afeta frequentemente atletas e esportistas, especialmente os goleiros que são propensos a quedas com trauma na anca.
A bursite trocantérica não é uma doença grave, mas pode evitar certas atividades para os doentes.
Geralmente os afetados são adultos ou idosos, raramente afeta as crianças.

Causas
A bursite trocantérica é causada por movimento exagerado dos tendões e fáscias sobre o trocânter maior,trauma, microtrauma repetitivo e a sobrecarga dos tendões que correm em torno da bursa . Pressão direta pode causar ou agravar os sintomas. Com a evolução da inflamação, a bursa progressivamente perde a sua função deslizante (“como um saco vazio”) e engrossa suas paredes.
Os pacientes com bursite trocantérica frequentemente apresentam uma ou mais das seguintes condições: doença na coluna lombar; diferença de comprimento entre os membros inferiores; doença na articulação sacroilíaca; artrose do joelho e entorse do tornozelo.
Acredita-se que estas anormalidades possam alterar a marcha e
consequentemente irritar a bursa trocantérica.
.Os desequilíbrios musculares e anatômicos podem contribuir para o nascimento da
doença, em particular: uma perna mais curta que a outra, a pelve em rotação ou
apoio incorreto do pé que causam atrito a nível da bursa.
Os exercícios incorretos ou simplesmente excessivos podem causar a doença
porque provocam um contínuo atrito sobre a estrutura.


Sintomas
Apesar de existirem mais de quatro bursas trocantéricas que podem ser afetadas, os sintomas são geralmente os mesmos independentemente da bursa afetada. A bursite trocantérica causa dor na lateral do quadril e na coxa, podendo causar dificuldade para caminhar. A pressão direta sobre a bursa aumenta a dor e é difícil deitar sobre o lado afetado. Por todas estas manifestações, a bursite trocantérica pode prejudicar o sono, evitar a realização de atividades físicas e reduzir significativamente a qualidade de vida.
Na
fase aguda é possível ver o paciente mancar ou com dificuldades para subir
escadas.
Os movimentos sem carga são dolorosos em adução e flexão do quadril além do ângulo direito, é possível uma limitação de amplitude do movimento.
As pontadas podem ser sentidas no glúteo, no abdômem direito ou esquerdo e na área externa da coxa.
Se não é curada, a bursite trocantérica pode tornar-se crónica ou persistente.

Epidemiologia e quadro clínico
As mulheres, em uma relação de 4:1 comparada com os homens, são mais freqüentemente afetadas, com a prevalência aumentada entre a quarta e sexta décadas de vida.
A dor é de característica crônica, intermitente sobre o aspecto lateral do quadril. Ocasionalmente, o início da dor é agudo ou subagudo, podendo ser intensa. Normalmente a dor piora a noite e o paciente tem dificuldade para dormir(8,10). A localização da dor é atrás e posteriormente ao trocânter maior, podendo se estender no aspecto lateral da coxa em 25 a 40% dos casos, e até a perna e tornozelo, mas não até o pé. Pode ser localizada também na região lombar baixa e, em alguns casos, ser acompanhada de parestesia na face lateral da coxa mas sem localização de dermátomo específico. A dor pode ser ainda provocada ficando-se na mesma posição por muito tempo ou quando o paciente deita-se contra o lado afetado.
Exame físico
A dor localizada na palpação em cima do grande trocânter pode ser encontrada em todos os pacientes sintomáticos. Tipicamente, esta área estará no local da inserção do glúteo médio. A dor pode ser reproduzida pela abdução ativa resistida e pela rotação externa e é provocada ocasionalmente pela rotação interna. Raramente a dor é reproduzida pela extensão do quadril. A ausência do movimento doloroso na flexão e da extensão do quadril ajuda distinguir a bursite trocantérica da doença intra-articular do quadril.
Mais da metade dos pacientes tem dor ao teste de Patrick-Fabere do quadril. O edema óbvio, como o perceptível no olécrano e na bursite pré-patelar, é incomum porque as bursas trocantéricas são estruturas relativamente profundas abaixo de alguns dos músculos mais volumosos no corpo. O exame físico pode também revelar a evidência de condições associadas tais como as doenças da coluna, artrite do quadril, a discrepância do comprimento dos membros inferiores, que devem ser sempre avaliadas.
Exames
Geralmente exames complementares não são necessários para o diagnóstico. Apesar disso, radiografias são solicitadas para excluir-se algumas doenças. Ultrassonografia, tomografia computadorizada e ressonância magnética são úteis em alguns casos para auxílio no diagnóstico, descartar outras doenças e guiar o tratamento.
A infiltração da bursa trocantérica também é útil no diagnóstico de alguns pacientes.
Figura 2 - Radiografia em ântero-posterior do quadril evidenciando calcificações em nível do grande trocânter.
Figure 2 - X-ray in anteroposterior hip showing calcifications in the level of the greater trochanter

Figura 3 - Cintilografia óssea demonstrando hipercaptação em nível do grande trocânter a direita.
Figure 3 - bone scan showing increased uptake level of the greater trochanter right.

Figura 4 - RM mostrando hipersinal na região do grande trocânter à direita.
Figure 4 - MRI showing hyperintense in the greater trochanter to the right area.

Tratamento da bursite trocantérica
O tratamento não cirúrgico da bursite trocantérica alcança resultados satisfatórios na maioria dos pacientes, incluindo o uso de medicações, fisioterapia e infiltrações. A resolução definitiva (“cura”) da bursite trocantérica pode ser difícil de ser alcançada em alguns casos, o que não significa que não haverá melhora dos sintomas com o tratamento.
As medicações são analgésicos e anti-inflamatórios. A fisioterapia associa medidas locais de temperatura com exercícios de alongamento dos tecidos que fazem pressão sobre a bursa. Alterações na marcha e função muscular também podem ser corrigidas pela fisioterapia em alguns casos. O uso de ultrassonografia terapêutica, estimulação elétrica percutânea (TENS) ou terapias por ondas de choque podem eventualmente ser indicados. A infiltração da bursa com anestésico e esteróide pode ser indicada quando as medidas anteriores não controlaram os sintomas.
A tratamento cirúrgico é indicado na minoria dos pacientes, naqueles em que os sintomas causam importantes limitações e o tratamento sem cirurgia não trouxe bons resultados. A cirurgia envolve a retirada da bursa inflamada e geralmente a liberação de tecidos (fáscias) causando pressão sobre a bursa trocantérica. Os tendões abdutores são avaliados e rupturas podem ser reparadas, da mesma forma que nos reparos de tendões do ombro. A cirurgia pode ser realizada de maneira tradicional, chamada aberta ou por videoartroscopia (endoscopia). A evolução nos materiais e técnicas têm permitido que procedimentos cada vez mais complexos sejam realizados através da videoartroscopia do quadril.
Exercícios de reabilitação e de alongamento podem ser úteis juntamente com o tratamento instrumental ou osteopatia para liberar o bloqueio das articulações.
A osteopatia pode ser útil porque melhora a circulação, desbloqueia as articulações e remove a compressão do nervo.
Se os tratamentos conservadores não são suficientes, você pode recorrer a cirurgia com excisão de líquido sinovial.
O melhor tratamento também inclui prevenção porque se você não excluir as causas primárias, a desordem certamente se repetirá.
Os exercícios devem ser adaptados as necessidades dos atletas, é necessário agir com:
Entre os possíveis esportes, a natação é permitida se não causa dor, enquanto o ciclismo pode piorar a inflamação, portanto deve ser evitao.
Não podemos determinar a duração da bursite trocantérica, em caso de lesão a dor pode ir em um curto espaço de tempo, mas em alguns casos torna-se crónica e se ela não for tratada, o tempo de recuperação pode ser de meses ou anos.
What is trochanteric bursitis?
The trochanteric bursitis is an inflammation that affects the synovial fluid of the greater trochanter of the femur.
The greater trochanter of the femur is essential in the dynamics of the lower limbs because it is the insertion of the extensor muscles (such as the large and small gluteus) and external hip rotators (eg piriformis).
There are three synovial bursae in the trochanter of the femur, which are:
These bursae act as if they were an "empty bag" on the bony prominences, facilitating sliding tendons and fascia on the bone. trochanteric bursitis is a common cause of pain in the hip and patients often suffer limitations in their physical activity and sleep with difficulty.
Between the greater trochanter of the femur and the fascia lata (the most affected)
Between the tendon of the gluteus maximus and the bone
Within the small gluteal tendon.
The bone surface is therefore the inflammation of the bursa is not deep.
The Trochanteric bursitis sa affects middle-aged and elderly people, and most often affects women subjects with imbalances in the body, for example, those with a shorter limb of the other (eterometria).
You have the same chance as bursitis occurs right or left, it is usually bilateral.
If the disease is caused by a trauma, you can break the capillaries, resulting in shedding of blood to the internal, in this case involves hemorrhagic bursitis.
The trocanterite includes trochanteric bursitis and enthesitis or insertional tendonitis of the muscles that are part of the greater trochanter, for example external hip rotators.
This disease often affects athletes and sportsmen, especially goalkeepers who are prone to falls and trauma hip.
The trochanteric bursitis is not a serious disease but can prevent certain activities for patients.
Generally those affected are adults or elderly, rarely affects children.
causes
The trochanteric bursitis is caused by excessive movement of the tendons and fascia of the greater trochanter, trauma, repetitive microtrauma and overloading of the tendons that run around the bursa. Direct pressure can cause or aggravate symptoms. With the evolution of inflammation, bursa gradually loses its sliding function ( "like an empty sack") and thickens the walls.
Trochanteric bursitis patients often have one or more of the following conditions: disease in the lumbar spine; difference in length between the lower limbs; disease in the sacroiliac joint; arthrosis of the knee and ankle sprain.
It is believed that these abnormalities can change the gait and consequently irritate the trochanteric bursa.
.the Muscular and anatomical imbalances can contribute to the birth of the disease, in particular: one leg shorter than the other, the pelvis rotating or incorrect foot support that cause friction within the bursa.
Incorrect or simply excessive exercise can cause disease because they cause a continuous friction on the structure.
symptoms
Although there are more than four trochanteric bursa can be affected, the symptoms are generally the same regardless of the affected bursa. The trochanteric bursitis causes pain in the hip and thigh, may cause difficulty walking. Direct pressure on the bursa increases the pain and it's hard to lie on the affected side. For all these manifestations, trochanteric bursitis can impair sleep, avoid physical activities and significantly reduce quality of life.
In the acute phase it is possible to see the patient limping or difficulty climbing stairs.
The movements are painful without charge in adduction and flexion of the hip and the right angle a movement range limitation is possible.
The twinges may be felt in the buttock, the right or left abdomen and the outer thigh area.
If not cured, the trochanteric bursitis can become chronic or persistent.
Epidemiology and clinical picture
Women in a ratio of 4: 1 compared to men, are most often affected, with increased prevalence between the fourth and sixth decades of life.
The pain is chronic, intermittent feature on the lateral aspect of the hip. Occasionally, the onset of pain is acute or subacute, and may be intense. Usually the pain worsens at night and the patient has difficulty sleeping (8.10). The location of the pain is back and subsequently the greater trochanter and may extend in the lateral aspect of the thigh in 25-40% of cases, and up the leg and ankle but not to the foot. It can also be located in the lower lumbar and in some cases, be accompanied by paresthesia on the lateral side of the thigh but no specific dermatomal location. The pain can be caused even staying in the same position for too long or when the patient lies down against the affected side.
Physical exam
The localized pain on palpation over the greater trochanter can be found in all symptomatic patients. Typically, this area is in the gluteus medius insertion site. Pain may be reproduced by resisted active abduction and external rotation and is occasionally caused by internal rotation. Rarely pain is reproduced by hip extension. The absence of painful motion in flexion and hip extension helps distinguish trochanteric bursitis of hip intra-articular disease.
More than half of patients have pain when Patrick-Fabere test the hip. The obvious edema, as noticeable in the olecranon and prepatellar bursitis, is unusual because the trochanteric bursa are relatively deep structures below some of the bulkier muscles in the body. Physical examination may also reveal evidence of associated conditions such as diseases of the spine, hip arthritis, the length discrepancy of lower limbs, which should be valued.
exams
Generally additional tests are not required for diagnosis. Nevertheless, radiographs are requested to be excluded for some diseases. Ultrasonography, computed tomography and magnetic resonance imaging are useful in some cases to aid in the diagnosis, rule out other diseases and guide treatment.
Infiltration of trochanteric bursa is also useful in the diagnosis of some patients.
Treatment of trochanteric bursitis
Nonsurgical treatment of trochanteric bursitis achieves satisfactory results in most patients, including the use of medications, physical therapy and infiltrations. The final resolution ( "cure") of trochanteric bursitis can be difficult to achieve in some cases, does not mean that there will be no improvement of symptoms with treatment.
The medications are analgesics and anti-inflammatories. Physical therapy combines local temperature measurements with tissue stretching exercises that put pressure on the bursa. Changes in gait and muscle function can also be corrected by physical therapy in some cases. The use of ultrasound therapy, percutaneous electrical stimulation (TENS) or therapies shock wave may possibly be provided. The infiltration of the bursa with anesthetic and steroid may be indicated when the previous measures did not control the symptoms.
The surgical treatment is indicated in the minority of patients, those in whom symptoms are important limitations and treatment without surgery did not bring good results. The surgery involves the removal of inflamed bursa and generally release tissue (fascia) causing pressure over the trochanteric bursa. The abductor tendons are evaluated and breaks can be repaired in the same way that the shoulder tendon repairs. The surgery can be performed in a traditional manner, by arthroscopy or open call (endoscopy). Developments in materials and techniques have allowed more complex procedures are performed by hip arthroscopy.
Rehabilitation exercises and stretching can be helpful along with the instrumental treatment or osteopathy to release the locking of joints.
The osteopathy can be useful because it improves circulation, unlocks the joints and removes nerve compression.
If conservative treatments are not enough, you can resort to surgery with excision of synovial fluid.
The best treatment includes prevention because if you do not delete the root causes, disorder certainly be repeated.
The exercises must be adapted to the needs of athletes, action is needed:
A better distribution of the periods of loading and unloading
Avoid certain very stressful exercises for bursa.
In this way, you have great benefits and avoid relapses.
Possible sports, swimming is permitted if it causes pain while cycling can worsen inflammation, so should be evitao.
How long bursitis of the hip? prognosis
We can not determine the length of time the trochanteric bursitis, in case of injury pain can go in a short time, but in some cases it becomes chronic and if it is not treated, the recovery time may be months or years.
fontes/ sources

Os movimentos sem carga são dolorosos em adução e flexão do quadril além do ângulo direito, é possível uma limitação de amplitude do movimento.
As pontadas podem ser sentidas no glúteo, no abdômem direito ou esquerdo e na área externa da coxa.
Se não é curada, a bursite trocantérica pode tornar-se crónica ou persistente.

Epidemiologia e quadro clínico
As mulheres, em uma relação de 4:1 comparada com os homens, são mais freqüentemente afetadas, com a prevalência aumentada entre a quarta e sexta décadas de vida.
A dor é de característica crônica, intermitente sobre o aspecto lateral do quadril. Ocasionalmente, o início da dor é agudo ou subagudo, podendo ser intensa. Normalmente a dor piora a noite e o paciente tem dificuldade para dormir(8,10). A localização da dor é atrás e posteriormente ao trocânter maior, podendo se estender no aspecto lateral da coxa em 25 a 40% dos casos, e até a perna e tornozelo, mas não até o pé. Pode ser localizada também na região lombar baixa e, em alguns casos, ser acompanhada de parestesia na face lateral da coxa mas sem localização de dermátomo específico. A dor pode ser ainda provocada ficando-se na mesma posição por muito tempo ou quando o paciente deita-se contra o lado afetado.
Exame físico
A dor localizada na palpação em cima do grande trocânter pode ser encontrada em todos os pacientes sintomáticos. Tipicamente, esta área estará no local da inserção do glúteo médio. A dor pode ser reproduzida pela abdução ativa resistida e pela rotação externa e é provocada ocasionalmente pela rotação interna. Raramente a dor é reproduzida pela extensão do quadril. A ausência do movimento doloroso na flexão e da extensão do quadril ajuda distinguir a bursite trocantérica da doença intra-articular do quadril.
Mais da metade dos pacientes tem dor ao teste de Patrick-Fabere do quadril. O edema óbvio, como o perceptível no olécrano e na bursite pré-patelar, é incomum porque as bursas trocantéricas são estruturas relativamente profundas abaixo de alguns dos músculos mais volumosos no corpo. O exame físico pode também revelar a evidência de condições associadas tais como as doenças da coluna, artrite do quadril, a discrepância do comprimento dos membros inferiores, que devem ser sempre avaliadas.
Exames
Geralmente exames complementares não são necessários para o diagnóstico. Apesar disso, radiografias são solicitadas para excluir-se algumas doenças. Ultrassonografia, tomografia computadorizada e ressonância magnética são úteis em alguns casos para auxílio no diagnóstico, descartar outras doenças e guiar o tratamento.
A infiltração da bursa trocantérica também é útil no diagnóstico de alguns pacientes.
Figura 2 - Radiografia em ântero-posterior do quadril evidenciando calcificações em nível do grande trocânter.
Figure 2 - X-ray in anteroposterior hip showing calcifications in the level of the greater trochanter
Figura 3 - Cintilografia óssea demonstrando hipercaptação em nível do grande trocânter a direita.
Figure 3 - bone scan showing increased uptake level of the greater trochanter right.
Figura 4 - RM mostrando hipersinal na região do grande trocânter à direita.
Figure 4 - MRI showing hyperintense in the greater trochanter to the right area.
Tratamento da bursite trocantérica
O tratamento não cirúrgico da bursite trocantérica alcança resultados satisfatórios na maioria dos pacientes, incluindo o uso de medicações, fisioterapia e infiltrações. A resolução definitiva (“cura”) da bursite trocantérica pode ser difícil de ser alcançada em alguns casos, o que não significa que não haverá melhora dos sintomas com o tratamento.
As medicações são analgésicos e anti-inflamatórios. A fisioterapia associa medidas locais de temperatura com exercícios de alongamento dos tecidos que fazem pressão sobre a bursa. Alterações na marcha e função muscular também podem ser corrigidas pela fisioterapia em alguns casos. O uso de ultrassonografia terapêutica, estimulação elétrica percutânea (TENS) ou terapias por ondas de choque podem eventualmente ser indicados. A infiltração da bursa com anestésico e esteróide pode ser indicada quando as medidas anteriores não controlaram os sintomas.
A tratamento cirúrgico é indicado na minoria dos pacientes, naqueles em que os sintomas causam importantes limitações e o tratamento sem cirurgia não trouxe bons resultados. A cirurgia envolve a retirada da bursa inflamada e geralmente a liberação de tecidos (fáscias) causando pressão sobre a bursa trocantérica. Os tendões abdutores são avaliados e rupturas podem ser reparadas, da mesma forma que nos reparos de tendões do ombro. A cirurgia pode ser realizada de maneira tradicional, chamada aberta ou por videoartroscopia (endoscopia). A evolução nos materiais e técnicas têm permitido que procedimentos cada vez mais complexos sejam realizados através da videoartroscopia do quadril.
Exercícios de reabilitação e de alongamento podem ser úteis juntamente com o tratamento instrumental ou osteopatia para liberar o bloqueio das articulações.
A osteopatia pode ser útil porque melhora a circulação, desbloqueia as articulações e remove a compressão do nervo.
Se os tratamentos conservadores não são suficientes, você pode recorrer a cirurgia com excisão de líquido sinovial.
O melhor tratamento também inclui prevenção porque se você não excluir as causas primárias, a desordem certamente se repetirá.
Os exercícios devem ser adaptados as necessidades dos atletas, é necessário agir com:
- Uma melhor distribuição dos períodos de carga e descarga
- Evitar certos exercícios muito estressantes para a bursa.
Entre os possíveis esportes, a natação é permitida se não causa dor, enquanto o ciclismo pode piorar a inflamação, portanto deve ser evitao.
Quanto tempo dura a bursite do quadril? O prognóstico
Não podemos determinar a duração da bursite trocantérica, em caso de lesão a dor pode ir em um curto espaço de tempo, mas em alguns casos torna-se crónica e se ela não for tratada, o tempo de recuperação pode ser de meses ou anos.
What is trochanteric bursitis?
The trochanteric bursitis is an inflammation that affects the synovial fluid of the greater trochanter of the femur.
The greater trochanter of the femur is essential in the dynamics of the lower limbs because it is the insertion of the extensor muscles (such as the large and small gluteus) and external hip rotators (eg piriformis).
There are three synovial bursae in the trochanter of the femur, which are:
These bursae act as if they were an "empty bag" on the bony prominences, facilitating sliding tendons and fascia on the bone. trochanteric bursitis is a common cause of pain in the hip and patients often suffer limitations in their physical activity and sleep with difficulty.
Between the greater trochanter of the femur and the fascia lata (the most affected)
Between the tendon of the gluteus maximus and the bone
Within the small gluteal tendon.
The bone surface is therefore the inflammation of the bursa is not deep.
The Trochanteric bursitis sa affects middle-aged and elderly people, and most often affects women subjects with imbalances in the body, for example, those with a shorter limb of the other (eterometria).
You have the same chance as bursitis occurs right or left, it is usually bilateral.
If the disease is caused by a trauma, you can break the capillaries, resulting in shedding of blood to the internal, in this case involves hemorrhagic bursitis.
The trocanterite includes trochanteric bursitis and enthesitis or insertional tendonitis of the muscles that are part of the greater trochanter, for example external hip rotators.
This disease often affects athletes and sportsmen, especially goalkeepers who are prone to falls and trauma hip.
The trochanteric bursitis is not a serious disease but can prevent certain activities for patients.
Generally those affected are adults or elderly, rarely affects children.
causes
The trochanteric bursitis is caused by excessive movement of the tendons and fascia of the greater trochanter, trauma, repetitive microtrauma and overloading of the tendons that run around the bursa. Direct pressure can cause or aggravate symptoms. With the evolution of inflammation, bursa gradually loses its sliding function ( "like an empty sack") and thickens the walls.
Trochanteric bursitis patients often have one or more of the following conditions: disease in the lumbar spine; difference in length between the lower limbs; disease in the sacroiliac joint; arthrosis of the knee and ankle sprain.
It is believed that these abnormalities can change the gait and consequently irritate the trochanteric bursa.
.the Muscular and anatomical imbalances can contribute to the birth of the disease, in particular: one leg shorter than the other, the pelvis rotating or incorrect foot support that cause friction within the bursa.
Incorrect or simply excessive exercise can cause disease because they cause a continuous friction on the structure.
symptoms
Although there are more than four trochanteric bursa can be affected, the symptoms are generally the same regardless of the affected bursa. The trochanteric bursitis causes pain in the hip and thigh, may cause difficulty walking. Direct pressure on the bursa increases the pain and it's hard to lie on the affected side. For all these manifestations, trochanteric bursitis can impair sleep, avoid physical activities and significantly reduce quality of life.
In the acute phase it is possible to see the patient limping or difficulty climbing stairs.
The movements are painful without charge in adduction and flexion of the hip and the right angle a movement range limitation is possible.
The twinges may be felt in the buttock, the right or left abdomen and the outer thigh area.
If not cured, the trochanteric bursitis can become chronic or persistent.
Epidemiology and clinical picture
Women in a ratio of 4: 1 compared to men, are most often affected, with increased prevalence between the fourth and sixth decades of life.
The pain is chronic, intermittent feature on the lateral aspect of the hip. Occasionally, the onset of pain is acute or subacute, and may be intense. Usually the pain worsens at night and the patient has difficulty sleeping (8.10). The location of the pain is back and subsequently the greater trochanter and may extend in the lateral aspect of the thigh in 25-40% of cases, and up the leg and ankle but not to the foot. It can also be located in the lower lumbar and in some cases, be accompanied by paresthesia on the lateral side of the thigh but no specific dermatomal location. The pain can be caused even staying in the same position for too long or when the patient lies down against the affected side.
Physical exam
The localized pain on palpation over the greater trochanter can be found in all symptomatic patients. Typically, this area is in the gluteus medius insertion site. Pain may be reproduced by resisted active abduction and external rotation and is occasionally caused by internal rotation. Rarely pain is reproduced by hip extension. The absence of painful motion in flexion and hip extension helps distinguish trochanteric bursitis of hip intra-articular disease.
More than half of patients have pain when Patrick-Fabere test the hip. The obvious edema, as noticeable in the olecranon and prepatellar bursitis, is unusual because the trochanteric bursa are relatively deep structures below some of the bulkier muscles in the body. Physical examination may also reveal evidence of associated conditions such as diseases of the spine, hip arthritis, the length discrepancy of lower limbs, which should be valued.
exams
Generally additional tests are not required for diagnosis. Nevertheless, radiographs are requested to be excluded for some diseases. Ultrasonography, computed tomography and magnetic resonance imaging are useful in some cases to aid in the diagnosis, rule out other diseases and guide treatment.
Infiltration of trochanteric bursa is also useful in the diagnosis of some patients.
Treatment of trochanteric bursitis
Nonsurgical treatment of trochanteric bursitis achieves satisfactory results in most patients, including the use of medications, physical therapy and infiltrations. The final resolution ( "cure") of trochanteric bursitis can be difficult to achieve in some cases, does not mean that there will be no improvement of symptoms with treatment.
The medications are analgesics and anti-inflammatories. Physical therapy combines local temperature measurements with tissue stretching exercises that put pressure on the bursa. Changes in gait and muscle function can also be corrected by physical therapy in some cases. The use of ultrasound therapy, percutaneous electrical stimulation (TENS) or therapies shock wave may possibly be provided. The infiltration of the bursa with anesthetic and steroid may be indicated when the previous measures did not control the symptoms.
The surgical treatment is indicated in the minority of patients, those in whom symptoms are important limitations and treatment without surgery did not bring good results. The surgery involves the removal of inflamed bursa and generally release tissue (fascia) causing pressure over the trochanteric bursa. The abductor tendons are evaluated and breaks can be repaired in the same way that the shoulder tendon repairs. The surgery can be performed in a traditional manner, by arthroscopy or open call (endoscopy). Developments in materials and techniques have allowed more complex procedures are performed by hip arthroscopy.
Rehabilitation exercises and stretching can be helpful along with the instrumental treatment or osteopathy to release the locking of joints.
The osteopathy can be useful because it improves circulation, unlocks the joints and removes nerve compression.
If conservative treatments are not enough, you can resort to surgery with excision of synovial fluid.
The best treatment includes prevention because if you do not delete the root causes, disorder certainly be repeated.
The exercises must be adapted to the needs of athletes, action is needed:
A better distribution of the periods of loading and unloading
Avoid certain very stressful exercises for bursa.
In this way, you have great benefits and avoid relapses.
Possible sports, swimming is permitted if it causes pain while cycling can worsen inflammation, so should be evitao.
How long bursitis of the hip? prognosis
We can not determine the length of time the trochanteric bursitis, in case of injury pain can go in a short time, but in some cases it becomes chronic and if it is not treated, the recovery time may be months or years.
fontes/ sources
http://portalbiocursos.com.br/ohs/data/docs/34/274_-_DoenYas_degenerativas_no_quadril_ocasionada_por_bursite_importYncia_da_fisioterapia_para_o_tratamento.pdf